Neck Pain Physiotherapy Near You in Surrey, BC: Causes, Treatment, and Natural Relief
- Fri Feb 13
A “herniated disc” is one of those diagnoses people hear and immediately picture a ruined back forever. That’s not how it usually goes.
A herniated disc can be painful and scary, especially when it triggers sharp leg pain (sciatica) or arm symptoms from the neck. But many people improve with the right plan, time, and sensible movement. The key is understanding what’s happening, spotting the situations that need urgent medical attention, and avoiding the common traps that slow recovery.
This article is general education, not personal medical advice. If you’re unsure what’s going on, get assessed by a regulated health professional.
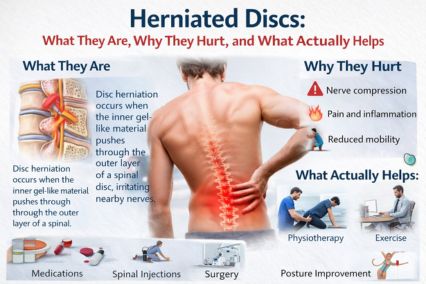
What is a herniated disc?
Your spine is built from vertebrae (bones) stacked with discs in between. Discs act like shock absorbers. Each disc has:
A herniated disc happens when part of the inner material pushes through a weakened or torn outer ring. If that bulge or herniation irritates a nearby nerve root, you can get nerve symptoms like pain, tingling, numbness, or weakness.
People call it a “slipped disc,” but discs don’t actually slip out of place. The issue is disc material changing shape and sometimes interacting with a nerve.
Disc bulge vs. disc herniation (and why the difference matters less than you think)
You’ll often hear:
On imaging (like MRI), both are common—even in people with no pain. Imaging findings don’t automatically explain symptoms. What matters most is the pattern: your history, your exam, whether symptoms match a specific nerve, and whether you’re improving over time.
Where herniations happen most
Lumbar (low back) disc herniation
This is the classic “back went out” story, often with sciatica (pain down the buttock/leg). The most common levels are L4-L5 and L5-S1, where the spine takes a lot of load and movement.
Cervical (neck) disc herniation
This can cause neck pain plus radiating arm pain, tingling, or weakness, often following a specific nerve distribution into the shoulder, arm, or hand.
Common causes and risk factors
A herniated disc is rarely one single moment that “ruined” your back. It’s usually a mix of:
Sometimes it happens with a specific lift or awkward movement. That doesn’t mean the disc is permanently “out.” It means the system was overloaded in that moment.
Symptoms: what people actually feel
A herniated disc can cause:
A simple rule: nerve-related pain often travels farther than muscle/joint pain and may come with sensory changes.
Red flags: when to seek urgent medical care
Most disc herniations are not emergencies. A small subset is.
Get urgent medical care now if you have:
These can signal serious conditions that need immediate assessment.
How a herniated disc is diagnosed
A good diagnosis is mostly clinical, not just an MRI result.
A physiotherapy assessment typically includes:
Do you need an MRI?
Often, not at first.
Imaging is usually considered if:
NICE guidance for low back pain and sciatica emphasizes appropriate assessment and management pathways rather than reflexively scanning everyone. NICE
Treatment that’s actually evidence-informed (and what to avoid)
There isn’t one magic exercise or one perfect posture. There is a smart process: calm symptoms down, keep you moving, reload the spine gradually, and restore confidence.
1) Keep moving, but stop “testing” it all day
Total bed rest usually backfires. Gentle movement helps maintain circulation, reduces stiffness, and keeps the nervous system from becoming more sensitive.
Good early options:
Bad early habit:
2) Calm the nerve down first, then build capacity
If you have sciatica or arm symptoms, the first goal is often symptom control:
A physio plan may include:
3) Medications (through your prescriber)
Some people need short-term medication support to keep moving and sleeping. That’s a discussion with your physician or pharmacist. NICE NG59 includes specific recommendations for sciatica and cautions against certain drug classes in some contexts. NICE
4) Injections: sometimes useful, not a cure
Epidural steroid injections can help some people by reducing inflammation around a nerve root. They don’t “put the disc back,” and results vary. They’re usually considered when pain is significant, limiting function, and not settling with conservative care.
5) Surgery: appropriate for specific cases
Surgery is not the default. But it can be the right call when:
Clinical guidelines for lumbar disc herniation with radiculopathy discuss both conservative pathways and surgical options, and note that many people improve over time even without surgery. University of Rochester Medical Center
How long does recovery take?
This is the honest answer: it depends on irritability, nerve involvement, and how well your plan matches your presentation.
Typical patterns:
Your goal isn’t “zero sensation immediately.” Your goal is clear functional progress: walking farther, sitting longer, sleeping better, moving more confidently, and reducing flare frequency.
What helps reduce recurrence
You don’t prevent disc problems by moving like a robot. You reduce recurrence by building capacity.
Practical long-term strategies:
FAQs (5)
1) Is a herniated disc the same as sciatica?
Not exactly. Sciatica describes symptoms along the sciatic nerve (leg pain, tingling, numbness). A herniated disc is one common cause of sciatica, but not the only one.
2) Will a herniated disc heal on its own?
Many cases improve over time, especially with sensible activity and a graded rehab plan. Some disc herniations reduce in size on imaging, and symptoms often improve even when the disc still looks “abnormal.” University of Rochester Medical Center
3) Should I rest or keep exercising?
Avoid complete rest. Keep moving within tolerable limits. Early on, think “calm and consistent” rather than intense workouts. As symptoms settle, progressive strengthening and conditioning usually matter more than stretching.
4) Do I need an MRI right away?
Not usually. If there are no red flags and your symptoms are improving, imaging often doesn’t change early management. MRI becomes more useful when symptoms persist, worsen, or if injection/surgery decisions are on the table. NICE
5) What are the signs I might need surgery?
Progressive weakness, severe persistent leg/arm pain that doesn’t improve with appropriate conservative care, or clear neurological deficits are common reasons for surgical consultation. Decisions should match your exam, imaging, and goals. University of Rochester Medical Center
References (3)